Mealtime Partners, Inc.
Specializing in Assistive Dining and Drinking Equipment
January 2012 Independent Eating and Drinking Newsletter
 |
January Topics:
|
||
|
Mealtime Partners Home Page Send a Comment or Suggestion |
|||
The Very Versatile Front Mounted Drinking System
Mealtime Partners develops products to meet independent eating and drinking needs that are currently not satisfactorily fulfilled. An example of a previously unavailable product that was developed by Mealtime Partners is the Front Mounted Drinking System. Because, many people who are unable to pick up a drink with their hands also have a limited ability to suck, they require a short straw from which to drink (instead of a long drink tube). This reduces the mounting possibilities for a drinking system. The system must be in front of the user and near to their mouth. The Front Mounted Drinking System, is a drink holder that is positioned to hold a drink container (cup, bottle, 12 oz. can, etc.) close to the user's mouth. Thus, the straw can be as short as necessary to facilitate easy suction for the user. An additional benefit of the Front Mounted Drinking System is that it is the easiest to clean of all Mealtime Partners drinking systems. Many of the containers it holds are disposable and thus do not require cleaning. Those that do, are usually easy to wash or are dishwasher safe.
In the process of creating these single purpose products, parts or components are often developed that are versatile enough to be used for more than one application. Our clamping products that were developed primarily to mount the Mealtime Partners drinking systems are an example of this. This article discusses the versatility of the Front Mounted Drinking System. However, when reading this article keep in mind that the Wheelchair Clamp used for this Drinking System can also be used in a wide variety of applications that do not necessarily relate to drinking.
The Front Mounted Drinking System is the most flexible of the drinking systems offered by Mealtime Partners. This is possible because it is a configuration of three components that are all adaptable: the Wheelchair Clamp, the Flex Arm, and the Cup Holder. The Front Mounted Drinking System is fundamentally a very versatile drink holder that can accommodate a variety of cups, cans, or bottles. It allows the drink to be held such that the drink tube (or straw) is very near the user's mouth. Thus the user can take a drink without using their hands with only a small amount of neck or upper body movement. Because the Clamp can be attached almost anywhere on the wheelchair and the Flex Arm can be bent to hold the Cup Holder in the desired position, the Front Mounted Drinking System becomes a semi-custom drinking system for each user.
Figure 1 below shows the Front Mounted Drinking System with a 24-inch Flex Arm mounted to the lower vertical support tubing of the wheelchair. The clamp is oriented horizontally on the tube. (The Front Mounted Drinking System can be purchased with 6-inch, 12-inch, 18-inch, 24-inch, or a 30-inch Flex Arm, as required to suit the needs of the user.)
 |
| Figure 1 - Front Mounted Drinking Systems Attached to Wheelchair |
To better understand how this system can be configured to accommodate the diverse needs of users, the three components used in the Front Mounted Drinking System will be discussed below.
The Wheelchair Clamp
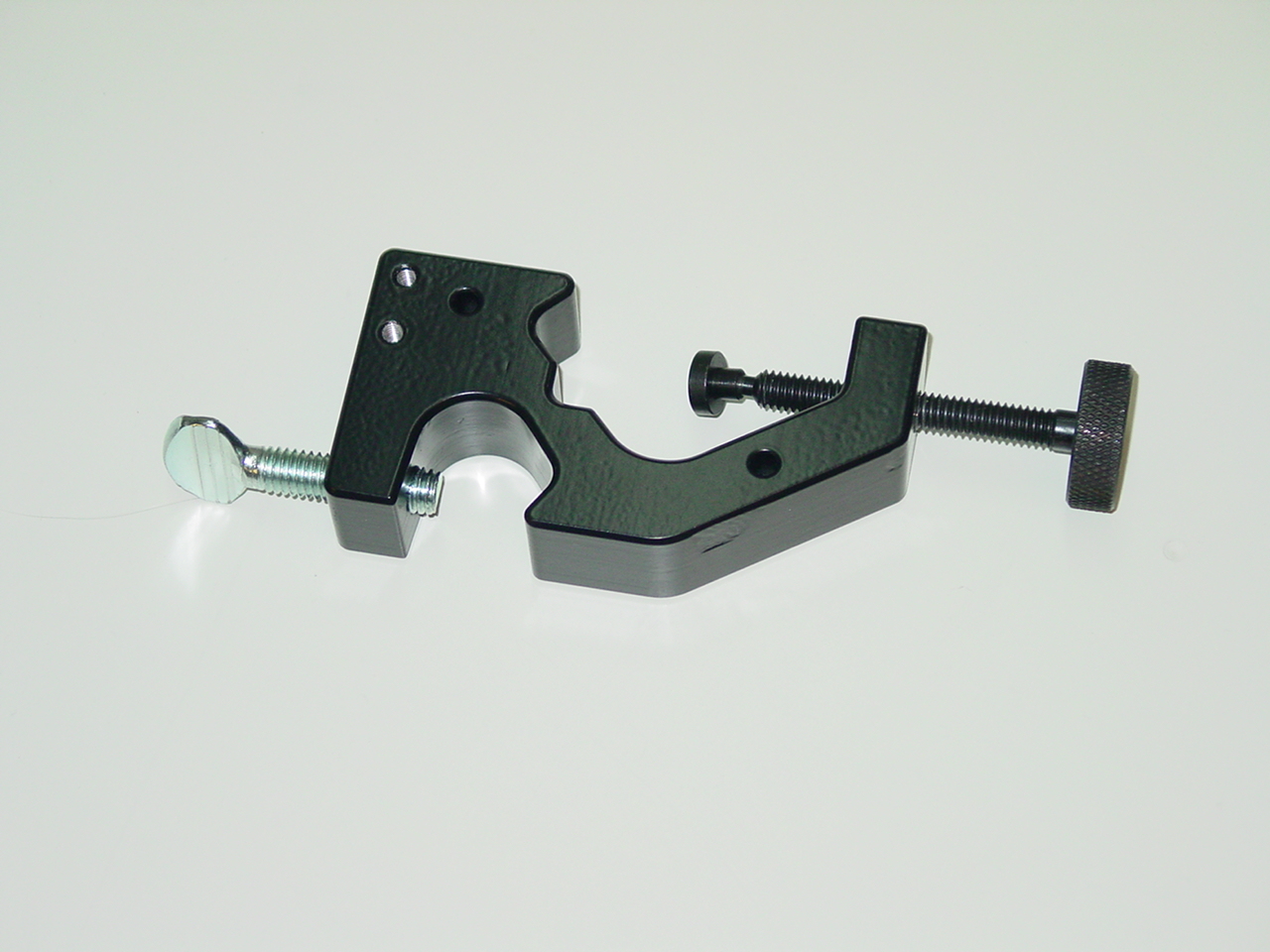 |
| Figure 2 - Photograph of the MtP Wheelchair Clamp |
The Wheelchair Clamp, shown in Figure 2, can be attached to round (i.e., tubular), or square surfaces. The opening can accommodate round objects ranging from 3/8 inch to 1-1/4 inches in diameter, and flat objects from 3/8 inch to 1 3/4 inches in diameter. This allows it to be attached to a variety of structural parts on a wheelchair frame, a bed rail, or a table top. And it can be clamped to both vertical and horizontal tubular or square rails. An integral part of the Wheelchair Clamp is its attachment holder which is opened and closed using a thumb screw. The built in attachment holder can hold shafts from 11/16 inch to 7/8 inch. For the Front Mounted Drinking System that is pictured above, this attachment holder with associated Thumbscrew facilitates holding the Flex Arm securely in position.
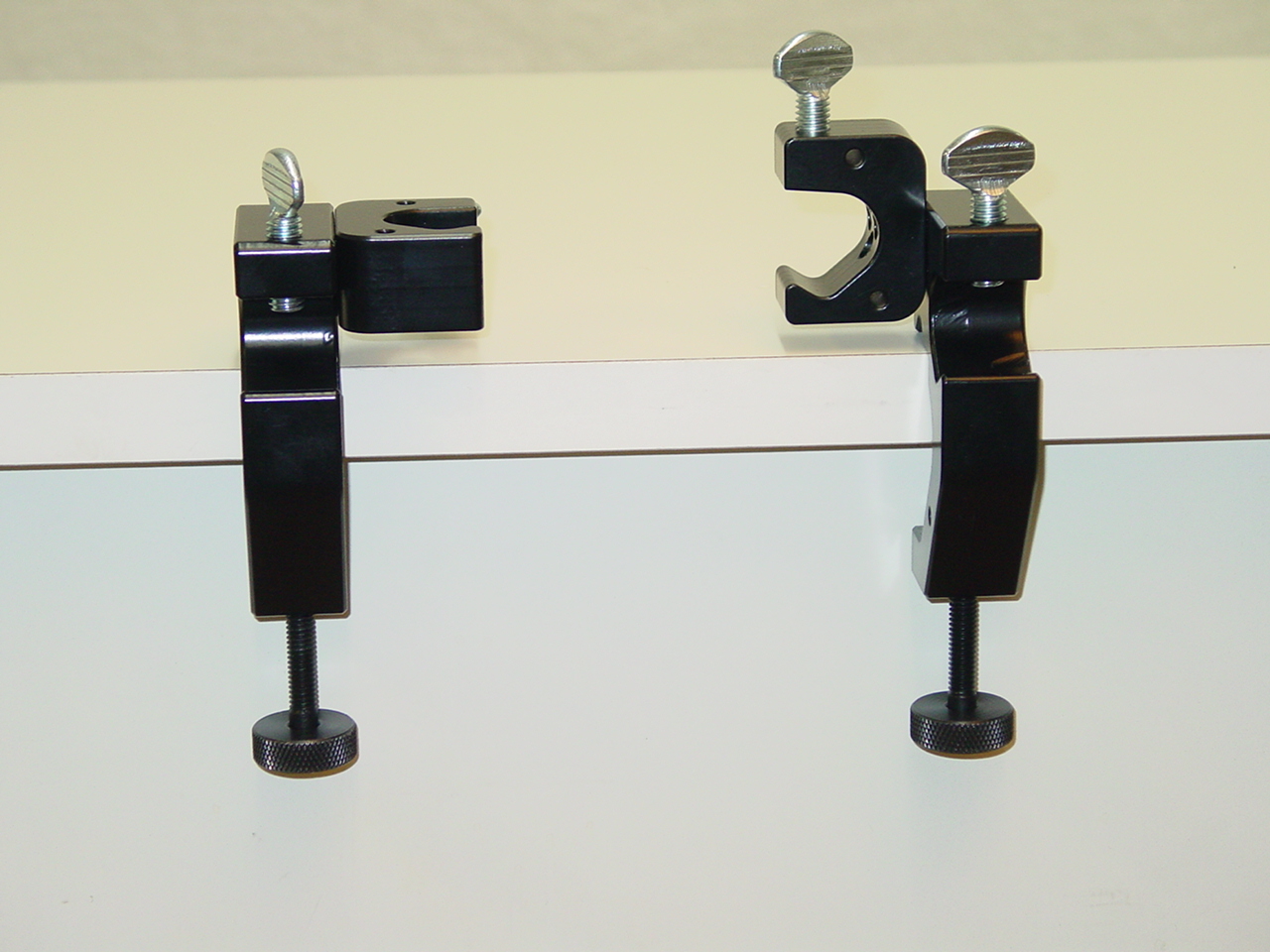
The photographs in Figure 3 show examples of different locations and orientations that the Flex Arm can be mounted on a wheelchair using the Wheelchair Clamp.
 |
 |
 |
| Figure 3 - Examples of Methods of Attaching the Front Mounted Drinking System to a Wheelchair | ||
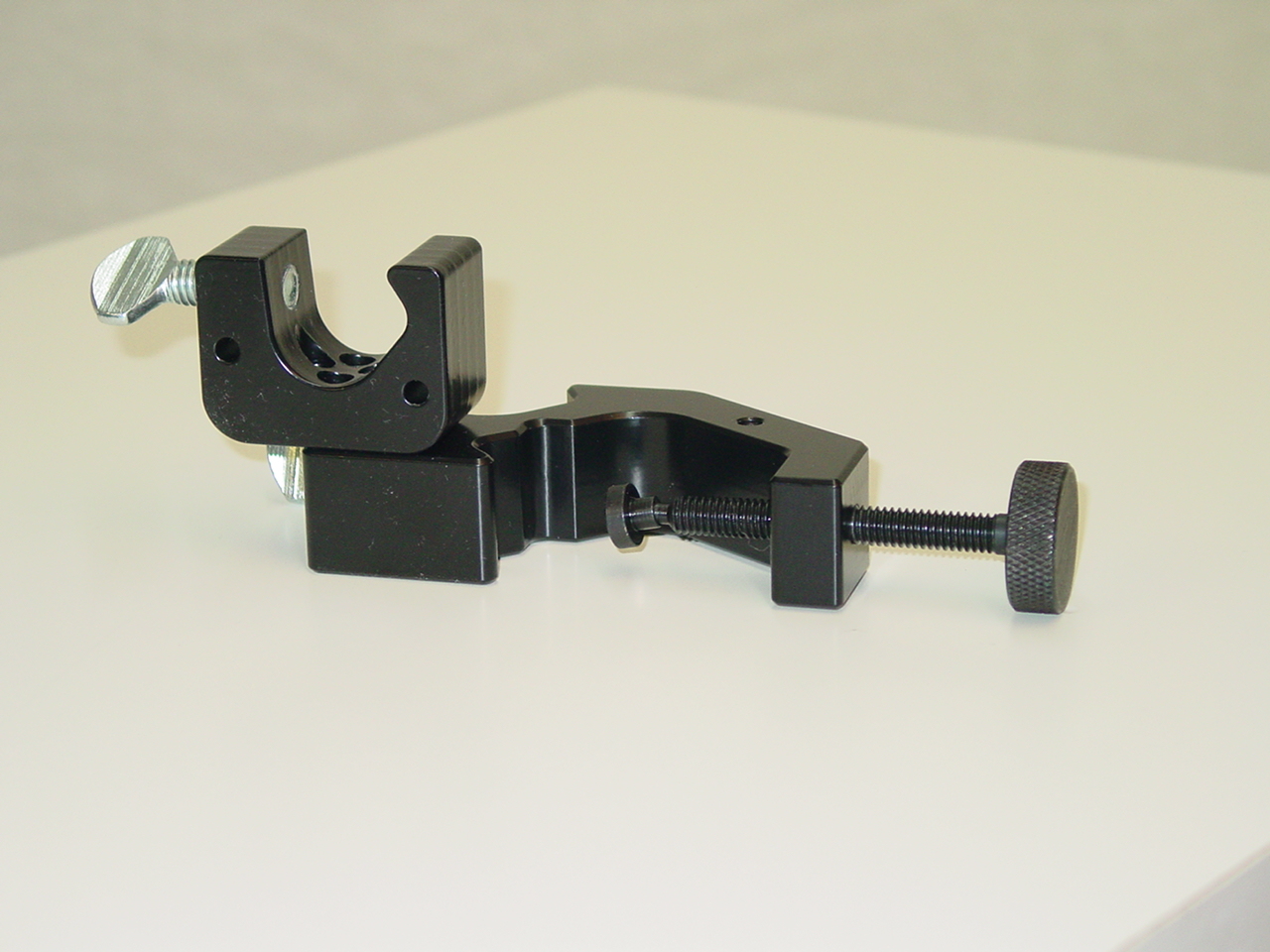
The Front Mounted Drinking System can also be mounted on a table top as shown in Figure 4 for users who do not wish to have their drink attached to their wheelchair but would rather roll up to the table and take a drink.
 |
| Figure 4 - The Front Mounted Drinking System can also be attached to a table. |
If the built-in attachment holder does not orient the flex arm in the desired direction for the user, or the user would like to attach two items (like a Flex Arm and a Flex Tube), a separate Attachment Holder can be added to the Wheelchair Clamp.
 |
 |
 |
| The MtP Wheelchair Clamp Attachment Holder | Attachment Holder Attached to Clamp | More ways for attaching the Attachment Holder |
| Figure 5 | ||
The Attachment Holder, pictured in Figure 5, can be oriented vertically or horizontally in relation to the Wheelchair Clamp and can be attached to either side of the Clamp. In the picture of the Front Mounted Drinking System attached to the edge of a table (Fig. 4), the built-in Attachment Holder is being used. However, had there been a need for the Flex Arm to extend vertically from the clamp, an auxiliary Attachment Holder could have been added to accommodate this positioning.
The Attachment Holder adds an additional value to the Wheelchair Clamp by allowing a second piece of equipment to be mounted using the clamp. The first piece of equipment can be held in position using the integral attachment holder and the second can be connected to the clamp using the auxiliary Attachment Holder. Examples of equipment that might be mounted simultaneously in this way are a Front Mounted Drinking System and a Sip N Puff control, or a Hydration Backpack with Drink Tube Positioning and an adaptive switch mount.
The Flex Arm
Mealtime Partners uses custom Flex Arms in many of their product assemblies. These Flex Arms are heavy duty, spring steel arms that have been chosen for their durability and capacity to maintain their position once they are positioned. Flex Arm (often referred to as flexible gooseneck tubing) can support an object and hold it in position. It is adjustable and can be re-positioned by bending. It is very rigid and will stay put after being re-positioned. The ends of the Flex Arm are solid shafts that are around 0.8-inch in diameter and 1-inch long so they can be clamped onto. Also, each end has a threaded hole (1/4"-20 thread), so objects can be screwed to it. Flex Arms are available in various lengths to accommodate different purposes. Currently Mealtime Partners provides products utilizing Flex Arms ranging from 6 inches in length to 30 inches in 6 inch increments.
The Cup Holder
The final essential component of the Front Mounted Drinking System is the Cup Holder. The Cup Holder attaches to the end of the Flex Arm and can be oriented in two directions, vertically or horizontally, as shown in Figure 6. Additionally, it should be noted that the Cup Holder has a cutout to accommodate the handle of a mug.
 |
| Figure 6 - Cup Holders with attachment bracket mounted both horizontally and vertically. |
The Cup Holder can accommodate a wide variety of drink containers ranging from standard 12 oz. cans and coffee cups to larger plastic cups as shown in Figure 7.
 |
 |
 |
| A Plastic Cup | A Water Bottle in a Koozie | A Coffee Cup |
 |
 |
 |
| A Soft Drink in a Koozie | A Small Plastic Cup in a Koozie | A Sports Bottle with a Drink Tube |
| Figure 7 - Front Mounted Drinking System Cup Holder Holding Various Containers | ||
A Koozie (which is provided with the Front Mounted Drinking System) can be inserted into the Cup Holder to position smaller cups snuggly (and to keep items hot or cold). Simply add a straw to the container and the drink is available.
In summary, the versatility of this drinking system allows it to be configured to meet the needs of a wide variety of users and make hydration easy and comfortable, even for individuals who lack the use of arms and/or hands. It requires the least suction of any drinking system currently available and is the easiest to clean because it can accommodate drink containers and straws that are disposable, or cups and bottles that can easily be removed and washed. Because of the previously described versatility of the components of the Front Mounted Drinking System, the Wheelchair Clamp and the Wheelchair Clamp Attachment Holder can now be purchased from Mealtime Partners as separate parts. The Wheelchair Clamp can support shafts, rods, and tubes from 3/8" to 1-1/4" diameter. The Wheelchair Clamp built-in attachment holder and the auxiliary Wheelchair Clamp Attachment Holder can support shafts, rods, and tubes from 11/16" to 7/8" in diameter. Using the Wheelchair Clamp and metal shafts or PVC pipes and other PVC parts (like elbows, T's, etc.) that are readily available from your local hardware store (Lowes, Home Depot, Ace, etc.), custom mounting systems can be readily constructed that will hold almost any item. For detailed information about these items or to purchase, click on the following links: Wheelchair Clamp, Wheelchair Clamp Attachment Holder.
| Did You Know? Did you know that the Food and Drug Administration (FDA) has begun testing all orange juice concentrate imported from Brazil. (Brazilian orange juice-concentrate accounts for around 10 percent of the U.S. supply.) This testing was implemented when low levels of an illegal fungicide called carbendazim were detected in imported Brazilian juice. The pesticide is banned in the U.S. but is used in Brazil to fight mold on citrus trees. The FDA says that low levels of carbendazim are not dangerous and they do not plan to recall any orange juice. However, they will stop any shipments of orange juice at the border that test positive for the fungicide. |
Autism and Difficulties with Eating
Autism is a relatively common developmental disorder. It is estimated to occur in 1 in every 1,000 births and occurs four times as frequently in boys as girls. Autism is typically diagnosed between the ages of 1 to 4 years and is characterized by speech and communication delays and difficulties; troubles with social behavior including failure to develop typical peer interactions and relationships; repetitive stereotypical behaviors and movement patterns; preoccupation with specific objects and intense interest in specific things, e.g., trains; non-typical interactions with toys, among other symptoms. Children with autism have sensory integration problems including being bothered by things that are rough on their skin (socks, shirts, underwear), loud noises, bright lights, smells, etc., and they like to have a routine and are distressed should a routine change. More information about autism can be found at many sites on the internet. NIH PubMed Health provides a thorough description. Also, the National Institute of Neurological Disorders and Stroke have an Autism Fact Sheet that includes a list of organizations that can provide more information.
It is not unusual for children who have a diagnosis of being on the autism spectrum to be described as picky or fussy eaters. In many cases the child is not just being a picky eater, as is common with many children as they evolve from being fed to becoming independent at mealtimes, they are exhibiting patterns of selective eating. (Selective eating is the clinical term for the little studied phenomenon of eating a highly limited range of foods, and being unwilling to try new foods.) Most children will outgrow this trait and become typical eaters; however, children with autism may carry their selective eating patterns into adulthood.
Children with autism, as compared with their peers who do not have autism, show a greater occurrence of refusing food and commonly have a significantly more limited range of food types that they are willing to eat. This restriction in the range of food that they eat can impact their nutrition. Food refusal appears to be exacerbated by the smell of food, its texture, its presentation on a plate or bowl, and whether foods that are served touch each other, etc. Children with autism may fixate on specific food and only be willing to eat that particular food. They may eat a very limited number of foods for a time and then abandon one and possibly select another food (but this doesn’t always happen). They may never be willing to eat the abandoned food again, or may after a time accept it again. If the food is never accepted again or replaced with another item, the repertoire of food selections is decreased significantly. For a parent this is devastating as they want their child to eat a healthy balanced diet and their child refuses to eat anything but the items they find acceptable. In many cases preference foods are sugary and fatty (for example, French fries and chocolate candy). Research has not yet identified why these items are more acceptable to children with autism than fruits, vegetables and other healthy foods. There is some anecdotal reporting that indicates that some children with autism improve both their behavior and their range of food choices when they adhere to a gluten free diet. As of now there is no clinical data to confirm this. A gluten free diet, as the name indicates, excludes foods containing gluten. Gluten is a protein found in wheat, barley, rye, malts and triticale, which is a hybrid of wheat and rye.
Regardless of the specific problems exhibited by children with autism, parents struggle ongoingly to have their children eat. The problem of feeding their child becomes much more complicated when the child enters school. In many cases children with autism will enter the school system before kindergarten through the Early Intervention Program. Thus eating becomes the domain of the teachers and paraprofessionals during the time that the child is in school. Parents are faced with the issue of sending preference food to school with the child and providing instruction for school staff regarding how the child chooses to eat (and having school staff astonished, or even horrified, by what is sent); or, by letting school staff provide the child with food prepared at school. For many children who have a very limited repertoire of food choices, school prepared food might be entirely unacceptable and the child may refuse to eat the entire time they are at school. However, some children may react differently in school than they do at home and may find some foods acceptable. How will school staff know how to select and present food? And, will they understand when a child finds what is being presented is objectionable? In such situations, the child may become more resistant or even throw a temper tantrum because they are stressed by the situation and the food that is being offered.
The situation can be compounded when the child needs someone to feed them or help them eat. Food presentation is such an important component of being fed for people with autism. This is worsened when someone is unable to express what they need their mealtime partner to do when they are being fed. In many cases the person feeding, whether it is a parent, a caregiver, or school staff, can make the mealtime a more stressful time because they are so concerned about having the child eat that they miss what the child is trying to communicate about their needs.
Because feeding problems are often complex and multi-facetted, parents are urged to seek the help of a pediatrician who may refer the child to a multidisciplinary feeding team for evaluation and treatment. The team will probably include a speech pathologist, a registered dietitian, an occupational therapist, and other clinicians as needed. They will help to plan interventions, or other techniques that can help bring an autistic child’s diet within the recommended nutrient levels for optimal growth and development. Many hospitals have clinics that specialize in treating feeding/eating problems. These facilities can help develop plans to lessen the difficulties experienced at mealtimes for both the child and parent, and facilitate the child developing skills that can allow them to enjoy and participate in meals with fewer difficulties. A list of some Feeding Clinics can be found at the end of this Newsletter.
Currently, many of these clinics are integrating Applied Behavior Analysis (ABA) therapy into their treatment plans to help them understand the triggers within the environment that cause tantrums or other undesirable behavior; and, to develop a strategy to help the child modify their behavior (go to http://www.lovaas.com for more information about ABA therapy). Clinicians will observe the relationship of a specific behavior to the environment and use ABA therapy to change the targeted behavior(s) by using simple, small instructional steps and reinforcement for positive responses from the child, with the hope and expectation that more appropriate behaviors will evolve. Parents are taught how to use ABA therapy and to carry the treatment home.
Many schools are also using ABA therapy within their programs as it has been shown to have positive outcomes for many students with autism. However, if the school that the child is attending does not currently use an ABA strategy, the parent should pass along to school staff the method that is working for the child at home and in therapy so that they can use the same strategies with the child. School based speech language pathologists can help teachers and paraprofessionals to support students with autism using strategies described in an article published by the American Speech-Language-Hearing Association, Language, Speech, and Hearing Services in School titled “Addressing Feeding Disorders in Children on the Autism Spectrum in School-Based Settings: Physiological and Behavioral Issues."
For many children the interface with another person at mealtimes can compound the behavioral difficulties that can be associated with eating. For those who are unable or unwilling to self-feed, the removal of the feeding partner can lessen the behavioral difficulties. The Mealtime Partner Dining System can provide a way for a child to self-feed, select the foods that they wish to, or are willing to eat and not have to deal with another person. Additionally, many children with autism enjoy technology and using adaptive switches and because of this trait, the Mealtime Partner Dining System can provide a positive experience relating to eating. For more information about the Mealtime Partner, click here.
 Pass the Peas Please
Pass the Peas PleasePeas aren't the easiest things to pick up, but the Mealtime Partner can reliably serve bite after bite of them if that’s what you want. If not, just move on to the next bowl and sample the pasta salad. The Mealtime Partner empowers its user to eat what they want, when they want it. To see a video of the Mealtime Partner Dining System, click here. To discuss how it might meet your specific needs, call us at 800-996-8607 or email us by clicking here. (Be sure to include your telephone number if you want us to give you a call.) |
The Mealtime Partner Dining System is quick and easy to learn and has no complicated programming requirements. Each Dining System comes with a complete training video on DVD so new users and caregivers can learn to use it in just a few minutes. To view a list of the instructional videos that may be selected by title, click here. The Mealtime Partner is by far the best assistive dining equipment ever developed. Before the engineering design team ever started, the design requirements for it were developed by a team of medical experts working with potential users. They examined the shortcomings in prior designs, the needs and desires of users, and the special requirements for providing safe and reliable operation in the various, often harsh, environmental settings where it must function. This resulted in the design of a dining system with quiet operation, that is easy to setup and use, easy to clean, has high durability (will last many years), serves food reliably, and is very safe to use. There are no other devices currently on the market that can even come close to matching its performance. For more information about the Mealtime Partner, click here. The Mealtime Partner meets the Medicare and Medicaid definitions of Durable Medical Equipment (DME). The United States Food and Drug Administration (FDA) categorizes the Mealtime Partner as a Class I type medical device. The Mealtime Partners has successfully completed all governmental electrical safety and electro-magnetic compatibility (EMC) compliance testing. |
List of Feeding Clinics:
Canada:
Rehabilitation Centre for Children Feeding Clinic
California:
LA Connections Project - Nutrition
University of Southern California/Childrens Hospital Los Angeles Affiliated Program
Los Altos Feeding Clinic Specializing in the Treatment of Pediatric Feeding Disorders
(650) 237-9111 or email pediatric_feeding@sbcglobal.net
Colorado:
The Children's Hospital of Denver Oral Feeding Clinic
Illinois:
Hope Children's Hospital - Feeding and Swallowing Clinic
Iowa:
University of Iowa Dept of Pediatric Gastroenterology
Florida:
University of Florida Shand's HealthCare Feeding Aversion Clinic
Georgia:
GI Comprehensive Feeding Clinic at Children's Healthcare of Atlanta
Maryland:
Kennedy Krieger Pediatric Feeding Disorders Continuum of Care
Massachusetts:
Feeding Team in Boston
Franciscan Children's Hospital Feeding Clinic
New York:
Children's Hospital of Buffalo - Feeding Disorders Clinic
New York University School of Medicine Multidisciplinary Feeding Clinic
North Carolina:
Carolina Pediatric Dysphagia
Pediatric and Adolescent Rehabilitation Outpatient feeding clinic and feeding program
Duke Children's Hospital and Health Center: Speech Pathology
Oregon:
Oregon Health and Science University Feeding Clinic
Ohio:
Pediatric Dysphagia management program at the Children's Hospital Medical Center of Akron
Cincinnati Children's Hospital interdisciplinary feeding clinic
Children's Hospital for Rehabilitation at the Cleveland Clinic - Feeding Disorders Program
Pennsylvania:
Children's Seashore House, Philadelphia - Feeding Program
The Children's Institute of Pittsburg - The Functional Feeding Program
Penn State Children's Hospital Feeding Evaluation Clinic
South Dakota:
South Dakota Children's Specialty Clinic - Feeding Clinic
Texas:
Children's Medical Center of Dallas - Pediatric Gastroenterology
Clinic 4 Kidz, Austin Texas
Washington:
Sacred Heart Medical Center Feeding and Growth Clinic
Virginia:
Children's Hospital of Richmond Pediatric Feeding Disorders Program
West Virginia:
West Virginia University Center for Excellence in Disabilities Feeding and Swallowing Clinic
UK:
University of Birmingham -- The Feeding Group
Mealtime Partners Website Navigation:
Home | Dining | Drinking | Videos | All Products | Warranty | Ordering | Calendar | FAQ | Newsletters | Contact
Please send comments and suggestions to newsletters@mealtimepartners.com
Copyright © Mealtime Partners, Inc. 2012
All rights reserved.