Mealtime Partners, Inc.
Specializing in Assistive Dining and Drinking Equipment
July 2012 Independent Eating and Drinking Newsletter
 |
July Topics:
|
||
|
Mealtime Partners Home Page Send a Comment or Suggestion |
|||
All of the products that Mealtime Partners, Inc. supplies and supports relate to swallowing because they are exclusively for dining and drinking. For this reason, the impact of providing food and liquid to those who use our products must be understood. The following article will provide some insight into specific aspects of swallowing relating to eating and drinking.
The following illustration shows the parts of the head and neck that are used in the various stages of swallowing.
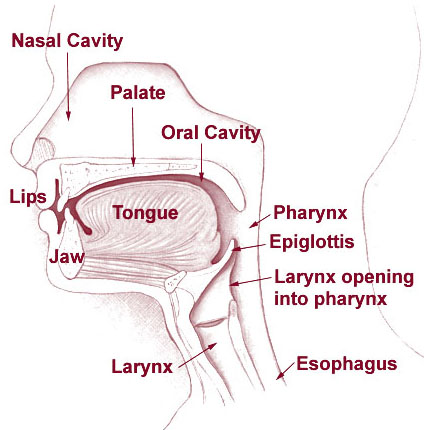 |
| Head and Neck Parts Used For Swallowing |
Swallowing is a complex task that involves the use of many muscles and nerves that must interplay perfectly for swallowing to be accomplished without difficulties. Parts of the process are voluntary and others are reflexive or controlled by the autonomic nervous system. The process of swallowing is made more complicated because the pharynx is a shared pathway used for solids and liquids during eating and drinking, and air during breathing. Eating/drinking and breathing must work separately from one another or the individual will choke or aspirate.
Swallowing happens in discrete phases beginning with food or liquid being placed in the oral cavity (the oral phase). The lips must open to allow entry of food or liquid into the mouth and then must close to contain what has been put into the mouth. Once something has entered the mouth, salivary glands become active. They produce saliva to moisten food that has entered the mouth. At the same time chewing takes place. The teeth are moved by the muscles that control the temporomandibular joint or jaw. Food is ground up by the teeth and moved from side to side of the mouth by the tongue. While this is happening the food is being mixed with saliva and is being formed into a ball, or bolus. Once a bolus is formed in the mouth it is ready to be swallowed. All of this action is voluntary.
When liquid is taken into the mouth it is also formed into a bolus. However, it does not require chewing. A small amount of liquid is formed into a ball in the middle of the mouth and then moved to the back of the mouth in anticipation of swallowing. If too big a volume of liquid is taken into the mouth initially it is broken into smaller portions prior to a bolus being formed so that a manageable amount of liquid can be swallowed each time. (More information about this phenomenon can be found in our July 2010 Newsletter article: Piecemeal Deglutination.)
To facilitate the bolus moving to the back of the mouth, the tongue presses against the hard palate and propels the bolus to the back of the mouth. At this point the swallow becomes reflexive and involuntary and the pharyngeal phase of the swallow initiates. For this phase to work properly all other activities of the pharynx (the throat) must stop, including chewing, breathing, coughing, etc. Muscles move various parts of the throat to allow the bolus to be swallowed safely, temporarily closing off passage to the nasal cavity (when this does not happen properly it is common to have liquids come out of the nose and coughing to be experienced). Additionally, the larynx is closed by the epiglottis covering it. When the larynx is closed, respiration is halted. This is known as swallow apnea and the length of the apneic event varies upon what is being swallowed, how long the person has been eating, and the person swallowing. There is no right or wrong amount of time.
The bolus then passes from the throat into the esophagus (the Esophageal phase of swallowing). It is moved downward by the muscles of the esophagus that contract and relax (peristaltic contractions) moving it through the esophagus to the stomach.
Typically a single swallow is relatively well controlled, but, as repeated swallows occur they can become less controlled and less organized, particularly if they are rushed or the person swallowing is tired. The above narrative provides a description of how a typical swallow is accomplished. However, it is impossible to know what is happening when someone swallows by simply watching them. The question arises how do you “troubleshoot” when you think someone is not swallowing properly? Once a physical examination has been conducted, a doctor may recommend that certain tests be performed. These tests may include:
An Esophagram or barium swallow. An esophagram is an x-ray or series of x-rays that are taken when a patient swallows liquid barium. The barium coats the lining of the esophagus and allows the radiologist to identify anatomical abnormalities and to see the movement of food and liquid as it passes through the esophagus. It is, however, limited in the information it can provide as only a few x-rays are typically taken to limit the exposure to radiation of the patient.
A Videofluoroscopy or videofluoroscopic swallowing study (VFSS). VFSS is an alternative to a barium x-ray. It provides a better visualization of a complete swallow. The patient eats and/or drinks barium laced food or liquid and a video x-ray is taken of the swallow from beginning to end. It allows the doctor to see the passage of food and liquid from the time it enters the mouth until it arrives in the stomach. Thus a clearer picture is provided of what is happening during a swallow. As with the esophagram, this test is limited by the amount of time that a patient can be exposed to radiation and provides only a short illustration of swallowing; it can show, however, the impact of thin liquids on the swallow as well as how solids are swallowed. For many people no irregularities are identified by these tests because they are performed in a highly controlled environment with a limited amount of food and/or liquid consumed. However, difficulties can exist as the person eats an entire meal or drinks a significant amount of liquid at one time.
A Gastrointestinal Endoscopy. A gastrointestinal endoscopy allows the doctor to see the inside of the esophagus and stomach. It is performed using a flexible fiber optic tube that has a tiny camera on the end of it. It allows the doctor to visualize the inside of the esophagus and thus identify abnormalities.
For most people, eating and drinking does not present any difficulties as long as they are provided enough time to pace their eating or drinking. When hurried, they do not chew adequately and may choke on lumps of food. If hurried when drinking, they may swallow too rapidly to allow the liquid to clear from their mouth prior to the next swallow. Some people are only able to swallow safely if the appropriate food textures and liquids of suitable thicknesses are provided. These types of problems frequently arise when someone is dependent upon another person to feed them or provide them with a drink. To lessen the occurrence of this problem for these people, they can be provided with assistive technology such as the Mealtime Partner Dining System for eating or a hands free drinking system for independent drinking. Additional Information about swallowing disorders can be found in the June 2012 Newsletter topic "Dysphagia".
| Independent Drinking | |
For most individuals, dehydration is 100% preventable. However, many people with disabilities suffer from some level of dehydration almost constantly. Mealtime Partners various drinking systems allow many individuals who are unable to use their hands to take a drink, to drink independently. For example, the Hydration Backpack Drinking System with Drinking Tube Positioning provides hands free drinking throughout the day for those who sit in a wheelchair and are unable to lift or hold a cup or glass. The drinking system is quick and easy to set up, the liquid container fits on the back of a wheelchair and the drinking tube can be positioned to meet the unique positioning needs of each individual. The Front Mounted Drinking System can position a variety of cups and drink containers very close to the users mouth for hands free drinking and allows a variety of other drinks to be made available throughout the day. For example, coffee in the morning, ice tea with lunch, a can of soda in the afternoon and a glass of milk before bed. The user drinks from their own container using a disposable straw. Because the straws and most of the containers can be disposed of or washed in a dishwasher, it is the easiest drinking system to clean. |
|
 The Hydration Backpack with Drink-Tube Positioning |
 The Front Mounted Drinking System |
Making liquid constantly available allows the user to drink whenever they want. This lowers the risk of dehydration and improves the quality of life for those who have one of these systems. For more information about all Mealtime Partners drinking systems and information about choosing the most appropriate drink system, click here. Click the following links for pricing and/or for ordering the Hydration Backpack Drinking System with Drinking Tube Positioning or the Front Mounted Drinking System. |
|
Considerations for Greater Enjoyment of Summer Foods
Now that summer is here many of us are changing our diet to include some of the bounties of the season. For children it is a wonderful opportunity to provide new taste experiences. However, for individuals who have difficulties with swallowing there are some considerations about preparation of these items and how they will be chewed and swallowed that should be noted when items are added to the diet.
Ice Cream: Is ice cream a liquid or a solid? Of course, it is both, but this presents some difficulties with making sure that it is safely swallowed. Before serving ice cream to someone who has oral motor difficulties, the first thing to consider is its temperature. For some people, the coldness of the ice cream can be helpful because it can “wake up” the taste buds. However, for many people, the coldness causes the taste buds to numb; therefore, consideration should be given to how each individual reacts to coldness in their mouth. The next issue that arises with eating ice cream is the fact that it melts. A spoonful of ice cream may be quite manageable in the mouth when it is solid, but as it melts and becomes a thin liquid, it may present problems for those who do not swallow thin liquids easily. To facilitate swallowing melted ice cream for those who aspirate thin liquids, add some crumbled up cookies. This provides a high calorie treat that is easier to control in the mouth.
Peaches or nectarines: Fruit is abundant at this time of year and is highly flavorful because of its freshness. The skin on many fruits can be difficult to chew and form into a bolus because it does not break down as easily as the flesh of the fruit. Therefore, it is helpful to peel the fruit (despite many of the nutrients being in the skin) to make eating them safe. Of course, if fruit is being pureed or blended, the skin can be included.
Tomatoes: Tomatoes are similar in preparation to many fresh fruits (as they are botanically a fruit). Attention should be paid to removing the seeds for individuals who have difficulties clearing food from their mouth or chewing small particles. Because of the shape and texture of the seeds they can easily “pocket” in the cheeks, around the gum line, or between teeth and can be difficult to remove. Seeds can be especially difficult to deal with for people with dentures and they can get stuck under the denture.
Melons: Summer time brings a magnificent assortment of different varieties of melons. Watermelons are easy to eat as they break down in the mouth without vigorous chewing. Because of the sugar content in a good watermelon, eating them will stimulate the production of saliva and, therefore, not only are they juicy but they cause salivation. An average watermelon is made up of 6% sugar and 92% water. It is a good source of vitamin C. Other types of melons commonly available in the United States include the cantaloupe and honeydew. The meat of these melons is firmer than that of a watermelon and requires more chewing, but is still relatively easy to eat.
Lemonade: Classic lemonade is a drink that is made from the juice of freshly squeezed lemons, sugar and water. The term lemonade is associated with many different types of drinks throughout the world and can mean a carbonated drink in many countries. Lemonade is a good source of vitamin C and acts as an antioxidant against environmental toxins. As far back as 460 BC it was known that lemon juice could cure scurvy, a disease that used to be common among sailors. Lemonade is an excellent drink to mask the flavor of thickening agents for those who need to have thin liquids thickened. Additionally, for those who have limited sense of taste, lemonade is easily “felt” inside the mouth and thus is able to be moved around the mouth and formed into a bolus more easily than less flavorful liquids.
Green beans: Along with the plethora of fresh fruits comes an assortment of fresh vegetables. Fresh green beans have a much bolder flavor than any that are preserved (weather frozen or canned). It should be noted that the skin or pod of fresh beans may have strings on one or both sides of the pod (thus they are often known as string beans). Also, beans that are left on the vine too long develop tough pod interiors that are difficult to chew and swallow. Even though, in general, the highest nutritional benefit is obtained from beans and other vegetables if they are only cooked briefly, they are easier to chew if they are cooked longer until they are soft.
All of the fresh produce available during summer months is an opportunity to explore new flavors and textures. For those who are unable to chew adequately to eat fruits and vegetables prepared in the standard manner, they can easily be finely chopped or blended and made into a Smoothy.
Regardless of any difficulties eating and swallowing, summer is a wonderful time to seek nutrition through fresh produce.
| Did You Know? Did you know that urinary tract infections (UTI’s) account for 8.3 million doctor visits each year in the United States? (Source: National Center for Health Statistics.) UTI’s, or bladder infections as they are more commonly known, occur more frequently in senior citizens because they have weakened bladder muscles due to the aging process, incontinence, and hold more urine in their bodies. This, along with their decrease in resistance to infection and reduction in mobility, makes them more susceptible. Thirty to forty percent of seniors with an infection do not show the typical sign of fever and, therefore, are harder to diagnose. Any rapid changes in behavior should be considered as an indicator of an infection, particularly changes in cognitive function. To avoid repeated UTI’s, everyone should be encouraged to drink at least two quarts of fluids, preferably water, per day (four quarts is better). It should be noted that many seniors and individuals with disabilities are reluctant to drink frequently because they will need to go to the bathroom frequently and must request help. Care providers should encourage frequent drinking and offer trips to the bathroom before they are requested. |
Mealtime Partners Website Navigation:
Home | Dining | Drinking | Videos | All Products | Warranty | Ordering | Calendar | FAQ | Newsletters | Contact
Please send comments and suggestions to newsletters@mealtimepartners.com
Copyright © Mealtime Partners, Inc. 2012
All rights reserved.